


On Being Trauma Informed in Practice, Pt I
Understanding the connection of addiction-trauma-persistent pain conditions that manifest with our patients and clients

Kihei, Maui April 2024
“Better is a morsel with quiet
than a house full of feast with strife.”
proverbs 17
Terry.
“Can you elaborate more on the comment you posted on my YouTube video on HERE11-Sidewalk. It seems quite insightful.” Glen
“Aloha!
In a quick nutshell, our life is trauma informed.
We are taught in our earliest years to disregard our own authenticity for safety and protection of parental figures… from an Interpersonal Biological sense ( social-neurosciences) we inhibit the pathways for salience and resilience by way of higher centers in the brain and thus we begin to use other means and methods to temporarily retrace back to what was right in feelings in our world when we were connected as whole to ourselves.
It is understanding our traumatic childhood experiences and how it has physiologically mapped maladaptive ways in which to cope.
So I say as mentor says,
“ What is right about addiction? "
What is it that one is receiving to feel at peace, whole, out of pain albeit for a brief moment with the addiction of choice.” ( Pain, work, shopping, social media, gambling, sex/porn, working out, food to name a few). For a mentor it was buying Classical CD’s while ignoring his doctors duties to deliver a newborn in L/D ( Labor and Delivery).
Chronic Pain is multifaceted. And in many cases the catalyst is found in forms of addictive personality traits and predilections through the trauma of early childhood programming and everyday life. Meaning Early, adverse childhood trauma experience may predict addiction as well as poorer health metrics. ( see ACES)
As Gabor Mate, MD posits so eloquently that at its core childhood traumas may be the wellspring of addiction through the loss of healthy attachment and embodiment of our own authentic nature over the need for this safety to be attached as a child.
The child essentially gives up their original and unique-authentic selves for the safety ( clothed, fed, sheltered) regardless of the potential harms that may come from conditions placed on the them to become part of the family, society, the culture.
In this the child becomes disciplined and taught to be someone else and turns against their very own uniqueness. This uniqueness will be sunken for some quite deeply unseen or known for the better part of life.
This is in part in the struggle to return we see in our own lives how we re-act life in maladaptive ways, by way of how we become emotionally charged by situations in relationship to another person. In many cases because we may have been taught that speaking up was in appropriate we may feel that anger for example was not a healthy emotion to display ( children are seen and not heard) and so we may have had to suppress anger and go against our natural tendency of self expression for attachment.
Glenn Lym is an Architect who also received his PhD in Social Psychology from Harvard. While he did not use it in a clinical sense it informed his practice in planning and creating space between lines on paper into the 3D scaled world. I believe it was a portal in a sense in understanding himself, his purpose and his true place in the world.
He and I met last week for a video call while I was on Maui researching my family ancestry. He is a 4th Generation Chinese American like me, twenty years my senior and in every-way just as youthful as I. This was our connecting point. He has put together a documentary of his ancestry’s march from Southern China to America as I am doing now in my own ancestry. He shared with me his work willingly.
This one particular documentary (above) was video’d from his office window down to the sidewalk in front of his office in his SOMA neighborhood.
For me I found reflections of how insidious and un-metabolized our traumatic life experiencing creates the world and shapes our way of moving into the world. A world that would not want nor have us, because we no longer fit or feel fit to reside in a “normal” existence.
I believe as Glenn does that we are bound as humanitarians in life and so would we endeavor to as he does. Caring does not have to be informed by our lack of love or authentic need for attention or our necessary needs taken and cared for. However, in my professional experience I am well aware that it is and in fact it is these injustices of traumatic experiences that may emblazon us boldly to be staunch advocates for the Humanitarian rights of others.
Why are we Touch Practitioners?
Why are we inclined to practice kindness as our daily motivation through touch and education?
In reference to Glenn’s documentary what does a couch, a tent and the hub-bub of a SOMA sidewalk life have to do with a Wise Practice?
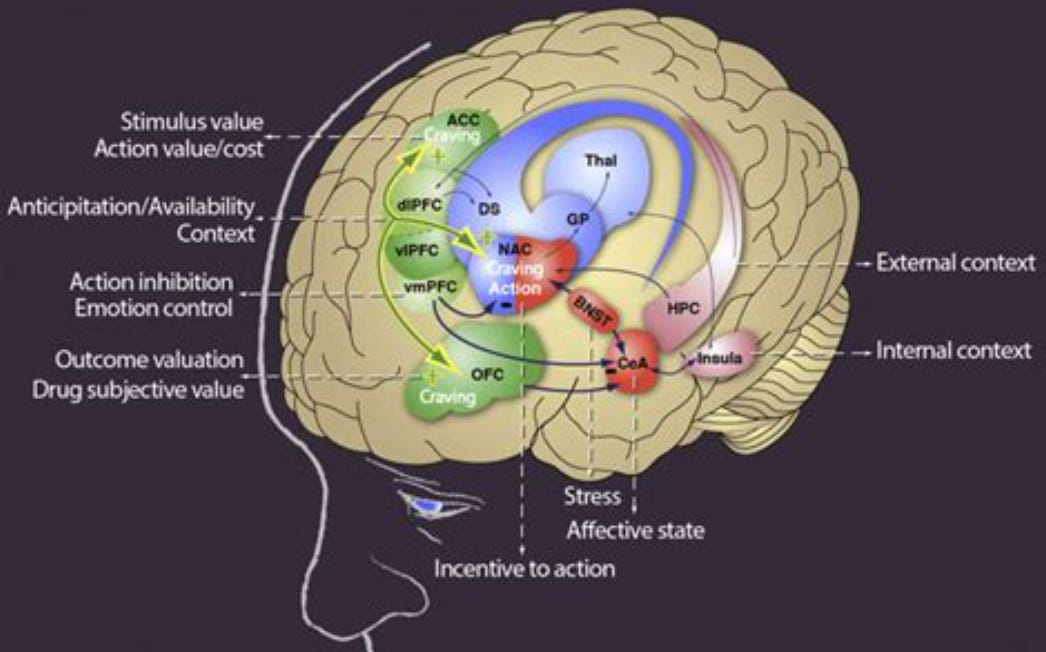
Two points I want to offer for those practicing at the table is to see clues of addiction through trauma from one perspective, within a neuro-physiologic lens. By understanding these mechanisms and pathways have it as a useful ally to heal from the cranial vault to the table, from the prefrontal cortex to the thalamus .
Chronic Low Back Pain reduces grey matter by 5-10%. This is equivalent to Grey Matter volume lost in 10-20 years of aging!
The dorsolateral prefrontal cortex (DLPFC) and orbito frontal cortex (OFC) are implicated in Chronic pain specifically.
The DLPFC has a top down influence and inhibitory control on limiting the magnitude of pain perception of pain by the OFC. Atrophy here in the DLPFC then loses this capacity and the variability in pain perception may be amplified on unequal measure to input. (allodynia)
The Thalamus has many nociceptive inputs, becoming a relay station of sorts as we may have learned in our Neuro classes back in school. These inputs make their way to the cortex and the shrinkage of grey matter may be a part of the answer to why Chronic Pain patients have a non dermatomal, vague, multi body area paresthesias and simply weird sensations.
Applying the Science to Our Practice
When we do our subjective assessment I encourage this place of inquiry once you have developed rapport and begun the task to address their concerns of pain relief to add into your examination. From a clinical sense without needing to have a PsyD we can deepen the therapeutic relationship with our patients and clients by:
Being specific on the question about stress. Ask them if work, home, financial and or interpersonal relationships has created more or less stress for them.
Being Trauma Informed. Study to understand the rootedness of persistent pain conditions as it relates to traumatic experiences in our childhood. No one escapes the harms of being unseen, unheard, and unfelt, socially dislocated in our unique selves.
To listen deeply and intensely as a Hawaiian elder I sat with on the 5 hour plane ride back from Maui stated to me is called “Hawk Medicine.” A laser focus on listening to understand through mercy, forgiveness and reconciliation. It quite literally is to be seen, heard and loved.
As I helped her up out of her middle seat she held my arm and looked me directly in the eyes and said, “Take our Aloha Spirit into your world and spread it. It is the only way to heal the travesty of our world today. Return to nature and exhalt in it and let it teach you the ways, but revere it as well. It is the only peaceful way, really.”
The art of listening is the ultimate healing tool any wise practitioner can master when it coincides with mercy and forgiveness. Her words and my deep reverence for the offering by her, this gentle, grounded homily reminded me that there is great need to turn our hearts outward and lead with Love.
To always lead with Love.
Blessings and Namaste,
t
Disclaimer: If you are not comfortable speaking about trauma then hold on this and begin to invest time and efforts to read and take workshops with these three notable folks. It, with some willingness, will change your life as it did mine.